Quick Summary
- Ischemic Stroke: Caused by a blockage (clot); accounts for about 87% of cases.
- Hemorrhagic Stroke: Caused by a bleed (rupture); accounts for about 13-15% of cases.
- Key Warning: Hemorrhagic strokes often present with severe headaches and higher immediate mortality.
- Prevention: Focuses on blood pressure control for bleeds and anticoagulants for clots.
- Urgency: Both require immediate emergency care; "Time is Brain."
The Big Divide: Blockage vs. Bleeding
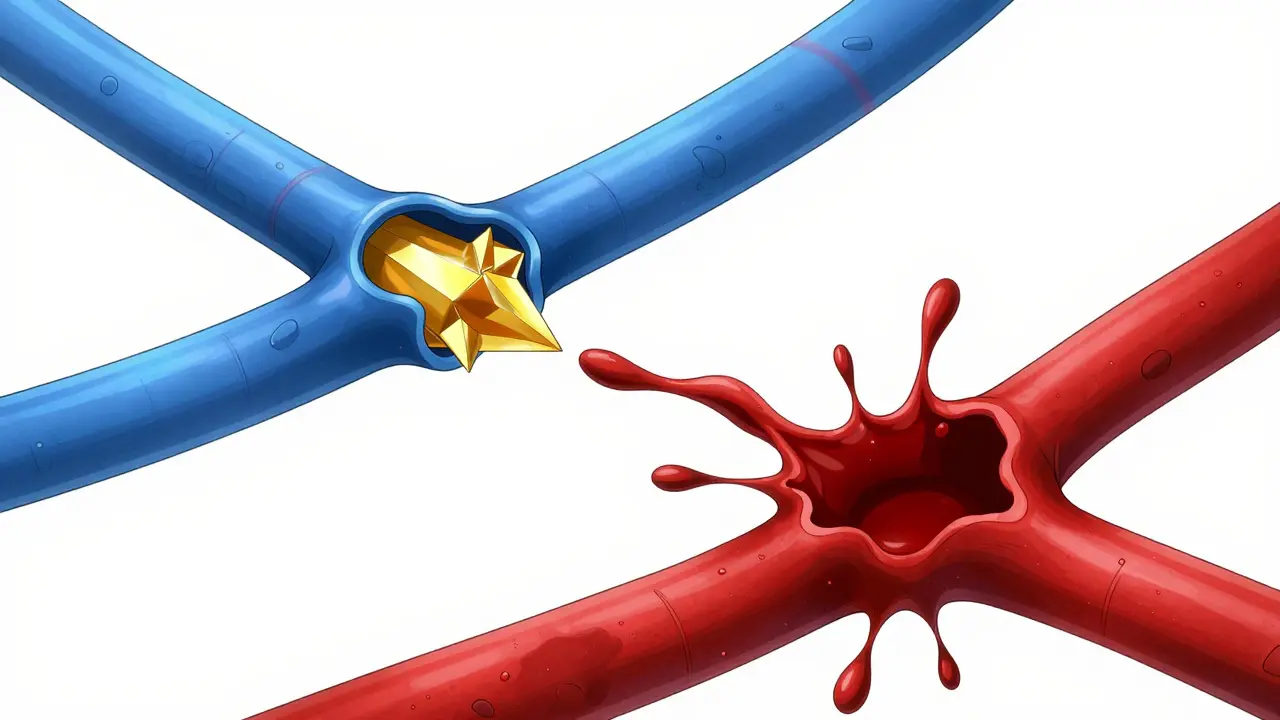
When we talk about Ischemic Stroke , we're talking about a plumbing problem where the pipe is clogged. Roughly 87% of all strokes fall into this category. A blood clot forms and cuts off the flow of oxygen-rich blood to your brain cells. If those cells don't get oxygen, they start to die within minutes. These blockages can happen right in the brain arteries or travel from elsewhere in the body, like the heart. On the flip side, a Hemorrhagic Stroke is more like a pipe bursting. Instead of a clog, a weakened blood vessel ruptures and leaks blood into or around the brain. While these only make up about 13-15% of cases, they are often more dangerous and immediately fatal because the leaking blood creates immense pressure inside the skull, crushing healthy brain tissue.Breaking Down Ischemic Strokes: Not All Clots are Equal
If you have an ischemic stroke, the "how" matters for your recovery. Doctors generally split these into a few main subtypes based on where the blockage started:- Thrombotic Strokes: These are the most common (about 50% of ischemic cases). A clot forms directly inside one of your brain's arteries, usually because of a buildup of fatty deposits called plaque.
- Embolic Strokes: Here, the clot is a "traveler." It forms somewhere else-often in the heart-and hitches a ride through the bloodstream until it gets stuck in a narrow brain artery. This is why Atrial Fibrillation (an irregular heart rhythm) is so dangerous; it can increase the risk of these embolic strokes by 500%.
- Cryptogenic Strokes: These are the medical mysteries. They make up about 30% of cases where, despite every test, doctors can't find the exact cause.
- Lacunar Strokes: These occur in the tiny, deep penetrating arteries. Because the affected area is small, the symptoms might be milder, but they still require urgent care.

Hemorrhagic Strokes: The Danger of Internal Pressure
When a vessel bursts, it doesn't just stop blood flow; it creates a physical mass of blood that puts pressure on the brain. There are two main ways this happens:- Intracerebral Hemorrhage: This is when a vessel ruptures deep inside the brain tissue. The biggest culprit here is chronic, uncontrolled high blood pressure, which weakens artery walls over years until they simply give way.
- Subarachnoid Hemorrhage: This happens on the surface of the brain. This is frequently caused by a Brain Aneurysm-a ballooning weakness in a blood vessel wall that eventually pops. This is often described by survivors as the "worst headache of my life."
Spotting the Difference: Symptoms and Warning Signs
While both types of stroke share the classic FAST signs (Face drooping, Arm weakness, Speech difficulty, Time to call 911), there are distinct patterns. If you're looking at a patient, the clues can be telling.| Symptom | Ischemic (Clot) | Hemorrhagic (Bleed) |
|---|---|---|
| Onset Speed | Often gradual (minutes to hours) | Sudden and dramatic |
| Severe Headache | Less common (approx. 19%) | Very common (approx. 92%) |
| Pupil Changes | Rare/Mild | Often dilated or unequal |
| Seizures | Rare | More frequent (approx. 17%) |
| Mental State | Confusion/Speech loss | High agitation/Loss of consciousness |
Treatment: Why the Diagnosis Must Be Exact
Here is the most critical point: You cannot treat a stroke until you know which type it is. Giving a "clot-buster" to someone with a brain bleed is like throwing gasoline on a fire-it will make the bleeding worse and could be fatal. This is why the gold standard is an immediate non-contrast CT scan to see if there is blood present before any meds are given. For ischemic strokes, the goal is to remove the blockage. Doctors use thrombolytic medications like Tenecteplase or Alteplase (tPA) to dissolve the clot. These must be given within a tight window-usually 3 to 4.5 hours after symptoms start. In severe cases, they may perform a mechanical thrombectomy, where a surgeon physically pulls the clot out of the artery. For hemorrhagic strokes, the goal is to stop the bleeding and reduce pressure. This might involve medications to lower blood pressure rapidly or surgical interventions. Two common procedures are "clipping" (placing a metal clip on an aneurysm) or "coiling" (filling an aneurysm with platinum coils to prevent it from rupturing further).
Prevention Strategies: Taking Control of Your Risk
Preventing a stroke depends heavily on which risk factors you have. While general heart health helps everyone, some strategies are more targeted than others.For Ischemic Risk: If you have atrial fibrillation, the priority is preventing clots from forming in the heart. Using anticoagulants (blood thinners) like warfarin or apixaban can slash your stroke risk by up to 70%. For those with high cholesterol or a history of mini-strokes, daily low-dose aspirin or clopidogrel can help keep the blood flowing smoothly.
For Hemorrhagic Risk: The absolute priority is blood pressure management. Keeping your systolic blood pressure below 120 mmHg can reduce the risk of a brain bleed by nearly 38%. When your blood pressure is chronically high, it puts constant stress on the small vessels in your brain, making them prone to rupture.
Lifestyle Wins: Some changes work for both types. Switching to a Mediterranean diet (rich in olive oil, nuts, and fish) has been shown to reduce overall stroke risk by 30%. Regular exercise-aiming for 150 minutes of moderate activity per week-cuts the risk by another 27%. And if you smoke, quitting is the fastest win you can get; your risk drops by half within just one year of stopping.
The Future of Stroke Care
We are moving away from "one size fits all" time windows. New research into perfusion imaging allows doctors to see exactly which parts of the brain are still salvageable, meaning some patients can now be treated up to 9 hours-or even 24 hours-after a stroke starts. Even more exciting are blood-based biomarkers. Imagine a quick blood draw in the ambulance that can tell paramedics with 92% accuracy whether a patient is having a bleed or a clot before they even hit the ER doors. This could shave critical minutes off the "door-to-needle" time, saving millions of brain cells in the process.Which type of stroke is more dangerous?
While ischemic strokes are far more common, hemorrhagic strokes generally have a higher immediate mortality rate. This is because blood leaking under pressure into the brain causes rapid damage and increased intracranial pressure. However, long-term recovery depends more on the overall severity of the stroke than just the type.
Can a mini-stroke lead to a major stroke?
Yes. A transient ischemic attack (TIA), often called a "mini-stroke," is a temporary blockage. It's a critical warning sign that your cardiovascular system is struggling. Many people who have a major ischemic stroke experienced a TIA days or weeks prior. Treating the underlying cause of a TIA can prevent a full-scale stroke.
Does aspirin prevent all types of strokes?
No. Aspirin is an antiplatelet medication that helps prevent ischemic strokes by stopping clots from forming. However, because it thins the blood, it can actually be dangerous for someone prone to hemorrhagic strokes, as it may increase the amount of bleeding if a vessel ruptures. Always consult a doctor before starting a blood-thinning regimen.
What is the "FAST" acronym?
FAST stands for Face drooping (one side of the face dips), Arm weakness (one arm drifts downward when raised), Speech difficulty (slurred or strange speech), and Time to call emergency services. Recognizing these signs within minutes is the single most important factor in improving survival and recovery rates.
Can lifestyle changes really prevent a stroke?
Absolutely. High blood pressure, smoking, and high cholesterol are modifiable risks. The SPRINT trial showed that aggressive blood pressure control significantly lowers bleed risk, while the PREDIMED study highlighted that a Mediterranean diet can reduce stroke risk by 30%. Combined with exercise and smoking cessation, these changes drastically alter your risk profile.
Comments
Kartik Agarwal
The emphasis on tPA and tenecteplase is spot on, but we should also discuss the nuances of neuroplasticity during the rehabilitative phase. For those navigating this, remember that the penumbra-that salvageable area around the infarct-is the primary target for these thrombolytics. Understanding the pathophysiology of cerebral perfusion pressure is key to maximizing functional outcomes post-event. Let's keep sharing these clinical insights to bridge the gap between acute intervention and long-term recovery.
On April 30, 2026 AT 00:15
Andrew Hanssen
It is quite quaint that the author assumes a non-contrast CT is the only definitive gold standard. While it is the first line, the nuance of MRI diffusion-weighted imaging is far superior for early ischemic detection. The oversimplification of the "pipe" analogy is merely an insult to the intelligence of the reader. I find this reductionist approach to be utterly exhausting.
On May 1, 2026 AT 02:00
SWATI NAWANGE
One must wonder why such rudimentary concepts are being presented as a revelation. The distinction between a thrombus and an embolus is basic medical literacy. It is truly tragic that the general populace requires such hand-holding to grasp the concept of intracranial pressure. This entire discourse is simply beneath the level of a first-year medical student, and yet, here we are, pretending this is enlightening information.
On May 2, 2026 AT 10:02
Tallulah Sandison
Just keep moving!! ❤️ Blood pressure control is such a win for everyone. Get out there and walk for those 150 mins!! You got this guys!
On May 3, 2026 AT 03:04
Bradley Gusick
Typical. They tell you to take "blood thinners" to save your brain, but who is actually funding the studies on the side effects? It's all a play by Big Pharma to keep us dependent on a pill every morning while they ignore the natural cures. We are living in a simulated reality where health is a commodity and the government decides who survives. Wake up people, the real cure is probably hidden in a vault somewhere while we follow these "guidelines" blindly.
On May 3, 2026 AT 09:28
Leah Sentz
This is why America is the best! 🇺🇸 Our medical tech like the mechanical thrombectomy is lightyears ahead of the rest of the world! 🚀 God bless our doctors who save lives every day! ❤️🇺🇸💪
On May 5, 2026 AT 02:19
Robert Cowley
Oh please, acting like a Mediterranean diet is some magic potion for your brain 🙄. I've seen people eat nothing but olives and still have a massive bleed because they're genetically predisposed. The data is just noise. It's all just a roll of the dice and we're just pretending we have control over our biology. 🤡
On May 5, 2026 AT 06:59
Christina Lancey
It is very helpful to have the FAST signs laid out so clearly. It might feel overwhelming to manage risk factors, but taking small steps toward a healthier diet can make a real difference for so many people.
On May 6, 2026 AT 14:55
Halle Dagley
The superiorty of American healthcare systems in managing these catastrophies is unparaleled. It is imperative that we maintain our ladership in medical reserch for the sake of the nation.
On May 6, 2026 AT 16:00
Rebekah Korak
You see, the tragedy of the human condition is that we try to quantify life and death through a table of symptoms, but the real struggle is the spiritual decay that manifests as physical illness. We obsess over the systolic pressure because we are terrified of the void, forgetting that the body is merely a vessel for a consciousness that doesn't care about plaque buildup. If you actually look at the intersection of mindfulness and vascular health, you'll realize that stress isn't just a risk factor, it's the very essence of the rupture. Most people are just walking deadlines because they refuse to align their energy with the universe, and no amount of apixaban is going to fix a soul that is fundamentally out of sync with its own existence.
On May 7, 2026 AT 01:25
Lando Neal
Wow!!! This is so helpful!!! I never knew the difference between the two types!!!
On May 8, 2026 AT 00:25