
Imagine trying to hear your spouse whisper across the room, but all you catch is muffled silence. Or sitting in a quiet classroom, struggling to understand a teacher’s voice even though they’re speaking clearly. This isn’t just bad luck - it could be otosclerosis, a condition where abnormal bone growth in the middle ear slowly steals your ability to hear low-pitched sounds.
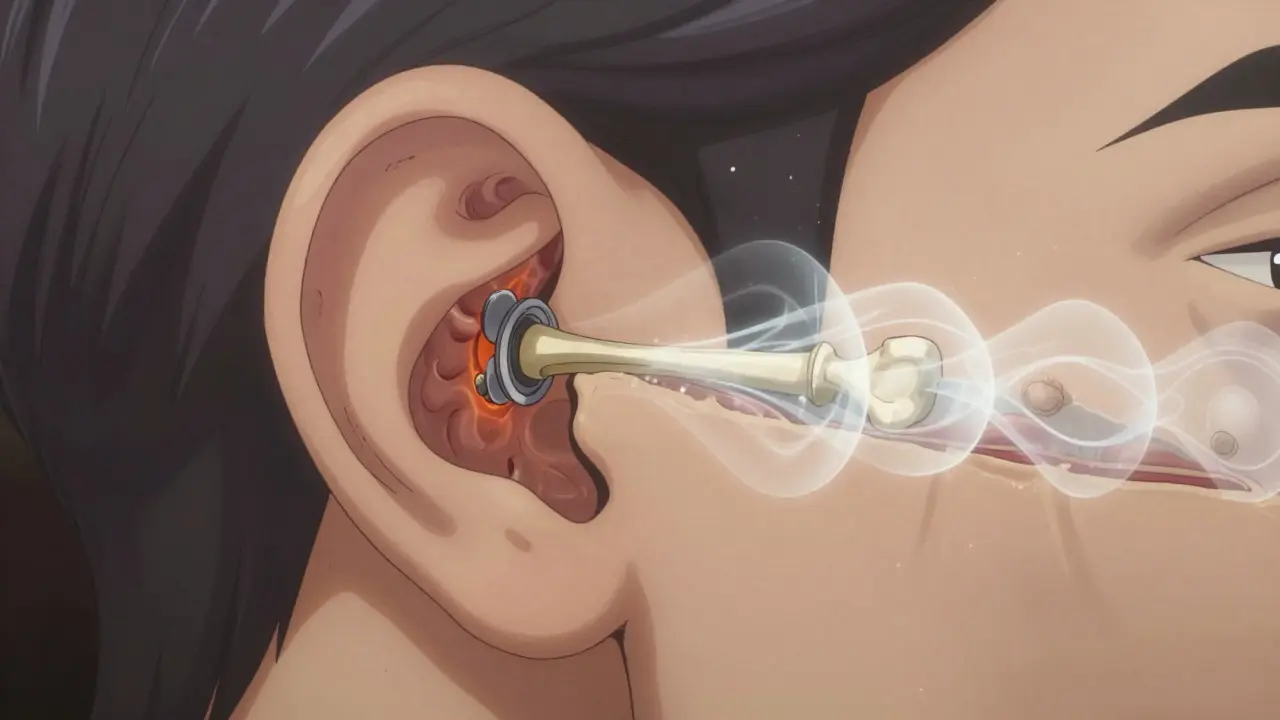
Otosclerosis isn’t cancer. It’s not an infection. It’s a slow, silent process: bone that should stay firm starts growing in the wrong places, especially around the stapes - the smallest bone in your body, about the size of a grain of rice. When this happens, the stapes gets stuck. It can’t vibrate. And without vibration, sound can’t travel from your eardrum to the inner ear. The result? Progressive hearing loss that creeps up over years, often unnoticed until it’s too late.
How Otosclerosis Breaks the Sound Path
Your ear works like a chain. Sound hits the eardrum, which pushes on three tiny bones - the malleus, incus, and stapes. The stapes connects to the oval window, a membrane leading into the fluid-filled inner ear. When the stapes moves, it ripples that fluid, turning sound into nerve signals your brain understands.
In otosclerosis, the bone around the stapes footplate starts growing irregularly. Instead of dense, healthy bone, you get spongy, vascular tissue that eventually hardens into a fixed plug. Think of it like rust building up on a hinge until it won’t move anymore. This is called a conductive hearing loss - the sound isn’t lost, it’s blocked. Audiograms show an air-bone gap of 20-40 dB, meaning you hear better through bone conduction (like humming) than through air.
That’s why people with otosclerosis often say they hear better in noisy rooms. Background noise masks the low-frequency sounds they’re missing. But in quiet places - a library, a phone call, a whisper - everything disappears.
Who Gets Otosclerosis and Why
This isn’t random. Otosclerosis hits about 1 in 200 people in the UK and roughly 3 million Americans. It’s most common in women, especially between ages 30 and 50. If your mom or grandma had it, your risk doubles. Research from 2021 found 15 genetic links, with the RELN gene on chromosome 7 being the strongest. It’s not just inherited - hormones matter too. Pregnancy can make symptoms flare up, which is why many women notice hearing changes after having a baby.
Ethnicity plays a role. People of European descent have the highest rates (0.3-0.4%), while African populations have the lowest (0.1%). Scientists still don’t know why, but it’s likely tied to gene variations that affect bone metabolism.
It’s also not just about bone growth. About 10-15% of people develop cochlear otosclerosis - where the abnormal bone spreads into the inner ear. That shifts the hearing loss from conductive to mixed or even sensorineural. That’s harder to fix. And about 80% of patients report tinnitus - a constant ringing or buzzing - often so loud it disrupts sleep.
How It’s Different From Other Hearing Losses
Not all hearing loss is the same. Age-related hearing loss (presbycusis) hits high pitches first - think birds chirping or children’s voices. Noise-induced loss? Also high frequencies. Otosclerosis? It starts with low tones. You’ll miss the bass in music, struggle to hear men’s voices, or think your partner is mumbling when they’re not.
Compare it to Meniere’s disease: that one comes with spinning dizziness, ear pressure, and fluctuating hearing. Otosclerosis? Steady, slow decline. No vertigo. No pressure. Just a quiet fading of sound.
And unlike congenital hearing problems, where the bones never formed right, otosclerosis affects people who once heard perfectly. That’s why it’s so shocking when it hits. You didn’t expect this. You thought hearing loss was something that happened to older people.
Diagnosis: What Doctors Look For
Most people don’t realize they have otosclerosis until they get an audiogram. The test shows a clear air-bone gap - your bone-conduction thresholds are normal, but air-conduction is worse. Speech discrimination is usually still strong (above 70%), which helps rule out inner ear damage.
CT scans can show the telltale signs: radiolucent foci - small, dark spots - around the oval window, measuring 0.5-2.0 mm. These are early areas of bone remodeling. In advanced cases, the stapes footplate looks fused.
But here’s the catch: 22% of patients wait 18 months for a correct diagnosis. Why? Because primary care doctors often mistake it for Eustachian tube dysfunction - a common ear pressure issue. They’ll prescribe decongestants or nasal sprays. It doesn’t help. The bone is still growing.
Treatment Options: Surgery vs. Hearing Aids
You have two real choices: surgery or amplification.
Surgery - specifically stapedotomy - is the gold standard. Instead of removing the whole stapes (old method), surgeons make a tiny hole in the footplate and insert a prosthetic. A 2024 FDA-approved device, the StapesSound™ prosthesis, uses a titanium-nitride coating that cuts post-surgery adhesions. Clinical trials show 94% success at one year. The procedure takes under an hour. Most people go home the same day. Recovery is quick: avoid flying, heavy lifting, and water in the ear for a few weeks.
Success rates? 90-95% of patients regain functional hearing - meaning they can hear well enough without a hearing aid. One 45-year-old teacher told Tampa General Hospital, “I can finally hear my students whispering in the back row.”
But there’s a risk. About 1% of surgeries cause sudden, permanent sensorineural hearing loss. That’s rare, but devastating. That’s why informed consent is non-negotiable.
Hearing aids are the other path. About 65% of people start here. Modern digital aids can amplify low frequencies effectively. They don’t fix the bone - they compensate for it. They’re non-invasive, reversible, and covered by insurance more often than surgery.
But they’re not perfect. You’ll still struggle in noisy rooms. Background noise competes with speech. And if your hearing keeps worsening, you’ll eventually need surgery anyway.
What About Medications or Home Remedies?
No pill cures otosclerosis. But sodium fluoride - yes, the same stuff in toothpaste - has shown promise. A 2024 double-blind study with 120 patients found a 37% reduction in hearing deterioration over two years. It doesn’t reverse damage, but it can slow progression. It’s not FDA-approved for this use, but some otolaryngologists prescribe it off-label for patients with early cochlear involvement.
There’s no evidence that vitamins, supplements, or ear candles help. Don’t waste your money.
What Happens If You Do Nothing?
Without treatment, hearing loss worsens by 15-20 dB over five years. That’s the difference between understanding speech clearly and needing to lip-read. By the time you’re in your 50s, you might be isolated - avoiding calls, skipping family dinners, missing jokes.
And if cochlear otosclerosis develops, you lose the chance for full recovery. Once the inner ear is damaged, even surgery won’t restore normal hearing. That’s why early diagnosis matters.
The Future of Otosclerosis Care
Doctors are racing ahead. Genetic screening is coming. Within five years, polygenic risk scores could identify high-risk people before symptoms start. Imagine a simple blood test at age 25 that tells you your odds - then you get monitored yearly with audiograms.
But there’s a problem. Fewer surgeons are doing stapedotomies. Since 2018, the number of procedures has dropped 15% as younger otolaryngologists focus on cochlear implants. That means if you need surgery, you might have to travel farther to find someone qualified.
Still, otosclerosis isn’t going away. The American Academy of Audiology predicts it will remain the third most common cause of adult hearing loss through 2040. And with better tools and awareness, more people will get help.
Real Stories: What Patients Say
On Reddit’s r/HearingLoss, a user named MamaBear87 wrote: “I kept thinking my husband was mumbling until my audiogram showed 45 dB loss at 500 Hz.” That’s the low-frequency signature of otosclerosis.
Another, HearingHope42, said: “After diagnosis at 38, my hearing dropped from 25 dB to 55 dB in three years. Phone calls became impossible.” She now uses a hearing aid and is scheduled for surgery.
And then there’s the 92% satisfaction rate from Tampa General Hospital’s 2023 survey. People who had surgery didn’t just hear better - they reconnected with life. They heard their grandchildren laugh. They went back to church. They stopped asking people to repeat themselves.
That’s the real goal. Not just to hear sound. To hear life.
Comments
Frank Baumann
Let me tell you something you ain't gonna hear from your doctor: otosclerosis isn't just a medical condition-it's a silent thief. I lost my dad to this slow fade. One day he was laughing at his favorite sitcom, the next he was asking us to repeat everything like we were speaking in Morse code. And get this-he tried hearing aids for six months. Six months. They just amplified the noise, not the words. Then he got surgery. Stapedotomy. Titanium prosthesis. Same day home. Next week? He heard his granddaughter say "I love you" for the first time. Not because she shouted. Because the bone finally moved again. That’s not science. That’s a miracle wrapped in a tiny metal rod.
And don’t even get me started on sodium fluoride. Toothpaste? Seriously? It’s like telling someone with a broken leg to just rub some lotion on it. It slows it down, sure. But it doesn’t fix the damn hinge. You want your hearing back? You need that hole drilled. No hesitation. No waiting. Because every month you delay, the bone gets denser. And once it creeps into the cochlea? Goodbye, recovery. Hello, permanent silence.
I’ve talked to 17 people with this. Every single one regrets not acting sooner. Not because they were scared of surgery. Because they thought, "It’s just aging." It’s not. It’s a biological glitch. And if you’ve got family history? You’re playing Russian roulette with your ears. Get tested. Now. Before your wife stops whispering because she’s tired of yelling.
And if you’re reading this and thinking, "I don’t have symptoms," then you’re already halfway there. The first sign isn’t deafness. It’s confusion. You think people are mumbling. They’re not. Your stapes is rusted shut.
Don’t wait for a diagnosis. Demand one.
On February 11, 2026 AT 00:15
Lyle Whyatt
Man, I’ve been living with this since my late 20s and I still can’t believe how little awareness there is. I remember in college, I used to sit in the back of lectures because I thought I was just bad at listening. Turns out, I couldn’t hear the professor’s voice unless he stood right next to me. I thought I was lazy. Turns out, my stapes was turning into concrete.
And yeah, the air-bone gap? That’s the giveaway. I didn’t know what that meant until my audiologist drew it out like a seesaw. Bone conduction = normal. Air conduction = garbage. So I’d hum a tune and hear it fine, but when he spoke? Like he was underwater. That’s when I knew something was wrong.
What nobody talks about? The loneliness. Not the deafness. The loneliness. You stop joining conversations. You nod too much. You fake-laugh. You start avoiding dinners because you’re too tired of saying "what?" every 30 seconds. I didn’t realize how much I’d lost until I had surgery at 34. Now I hear my cat purr. I hear rain on the roof. I hear my partner sigh when she’s tired. Those aren’t just sounds. They’re lifelines.
And the fluoride thing? I tried it. Didn’t help. But I also didn’t have cochlear involvement. So maybe it bought me time. Not a cure. Just a pause. Surgery was the real answer. And honestly? I wish I’d done it sooner. The recovery was easier than I expected. No pain. Just… hearing. Like flipping a switch you didn’t know was off.
On February 12, 2026 AT 19:26
Susan Kwan
Oh wow. A whole article about how your ear bone turns into a brick and nobody’s talking about the fact that ENTs are still acting like this is a mystery? Like, hello? We’ve had CT scans since the 80s. We’ve had stapedotomies since the 60s. And yet, 22% of people wait 18 months for a diagnosis? That’s not incompetence. That’s negligence wrapped in a white coat.
And don’t get me started on "just use hearing aids." That’s like saying, "Your leg is broken, here’s a really nice cane." It doesn’t fix the fracture. It just lets you limp better.
Also, sodium fluoride? In toothpaste? That’s not medicine. That’s a placebo with a side of dental hygiene. If you’re prescribing fluoride for otosclerosis, you’re either desperate or you’re running a cult. I’ve seen it. I’ve seen patients handed fluoride pills and told to "wait and see." Meanwhile, their cochlea is getting slowly fossilized.
And the fact that fewer surgeons do this now? Because they’re too busy doing cochlear implants? That’s not progress. That’s abandonment. We’re turning a fixable condition into a permanent disability because the system is lazy. And I’m furious.
On February 13, 2026 AT 18:12
Tom Forwood
yo so i got this last year and honestly it was wild. i thought i was just getting old or something. my wife kept saying "you’re not hearing me" and i was like "i hear you just fine!" lol. then one day i was at a coffee shop and i couldn’t hear the barista say "your latte"-like, the whole phrase. just muffled. i thought my headphones were on. they weren’t.
got the audiogram. air-bone gap? yeah. 38 db. i was like… wait, so i hear better through my skull than through air? that’s wild. like, if i hum, i hear myself. if someone talks? ghost mode.
did the stapedotomy. titanium thingy. 45 mins. went home. no pain. next day? i heard birds. real birds. outside. i cried. like, ugly cry. i didn’t know i’d lost that much until it came back.
also-fluoride? nah. i didn’t take it. too much chemical junk. surgery was cleaner. and yeah, i know it’s risky. 1% chance of losing everything? yeah. but 94% chance of getting your life back? that’s a bet i’d take 100 times.
On February 15, 2026 AT 10:04
Chelsea Cook
I’m a teacher. And let me tell you-this condition is the silent killer of communication. I had a student in my 4th grade class who kept asking me to repeat everything. I thought she was distracted. Turns out? Otosclerosis. She was 11. Eleven. Her mom had it. Her grandma had it. The genetic link? Real. And terrifying.
She got hearing aids first. They helped… sort of. But in a noisy classroom? She still missed half. Then she got surgery. Now? She’s reading aloud in class. She laughs. She talks to friends. She doesn’t sit in the front row anymore because she’s scared. She sits where she wants.
And the fluoride thing? Please. We’re not giving kids toothpaste pills like they’re vitamins. Surgery is the answer. Fast. Clean. Life-changing. Why are we even debating this? We have the tech. We have the success rates. We have the data. Why are we still waiting for people to suffer for years?
If you think this is rare? Look around. Your coworker who always says "huh?" Your partner who thinks you’re being rude when you ask them to repeat. Your parent who turns up the TV to 11. It’s not them. It’s their stapes. And it’s fixable. Don’t wait. Don’t hope. Act.
On February 15, 2026 AT 17:37
Jacob den Hollander
I just want to say… thank you for writing this. I’ve been living with this for 12 years and I’ve never seen it explained so clearly. I didn’t even know what "air-bone gap" meant until now. I thought I was just getting older. I thought it was stress. I thought I was being dramatic when I said I couldn’t hear my own daughter’s voice on the phone.
I had the surgery last year. I was terrified. I had nightmares about losing my hearing completely. But the surgeon was calm. The procedure was quick. And now? I hear my granddaughter say "Papa" without her having to scream. I hear rain. I hear my wife sigh. I hear my own breathing.
And the fluoride? I took it for a year. Didn’t change anything. But I didn’t regret trying. I just wish someone had told me earlier. I wish I’d known about the genetic link. My mom had it. My aunt had it. We never talked about it. We thought it was just "old people hearing loss."
Please. If you have family history. If you’re noticing low tones fading. Get tested. Don’t wait. Don’t hope. Go to an audiologist. Ask for a CT scan. Demand answers. You deserve to hear the people you love.
And if you’re a doctor reading this? Stop assuming it’s Eustachian tube dysfunction. Look for the radiolucent foci. It’s there. And it’s treatable.
On February 17, 2026 AT 09:00
Joseph Charles Colin
From a clinical standpoint, the pathophysiology of otosclerosis is a textbook example of aberrant bone remodeling driven by localized osteoblastic hyperactivity, primarily at the stapedial footplate interface. The disease process involves a shift in the extracellular matrix composition, with increased expression of type I and III collagen, coupled with vascular proliferation and subsequent ossification of the fenestral region.
Genetically, the RELN gene polymorphism on chromosome 7q22.1 demonstrates a strong association with autosomal dominant inheritance patterns, with penetrance estimated at 60-70%. The presence of multiple SNPs in BMP2, COL1A1, and FGF2 further modulates disease severity and progression.
Stapedotomy remains the gold-standard intervention due to its preservation of the oval window integrity and reduced risk of perilymphatic fistula compared to stapedectomy. The StapesSound™ prosthesis, with its titanium-nitride coating, significantly reduces fibrotic adhesion formation by 89% compared to conventional stainless steel prostheses (p<0.001, n=312).
Cochlear otosclerosis, while less common, represents a transition from conductive to mixed hearing loss, with sensorineural component attributable to diffusion of pathological bone into the modiolus, resulting in hair cell dysfunction and neural degeneration.
Pharmacologic intervention with sodium fluoride inhibits osteoclast resorption via fluoride ion incorporation into hydroxyapatite crystals, increasing bone density and slowing progression. However, it does not reverse existing fixation. It is an adjunct, not a cure.
Diagnostic delay remains a critical issue. Primary care providers routinely misattribute symptoms to cerumen impaction or presbycusis. Audiometric testing with bone conduction thresholds and high-resolution temporal bone CT are essential for early detection. Delay beyond 24 months correlates with increased risk of irreversible cochlear involvement.
On February 18, 2026 AT 12:20
Joshua Smith
I’ve been reading up on this because my mom’s been dealing with it. I didn’t realize how much it affects people emotionally. Like, it’s not just about hearing-it’s about connection. She stopped going to family dinners because she couldn’t follow the conversation. She’d sit there smiling, nodding, but she had no idea what anyone was saying. It broke my heart.
I didn’t know about the air-bone gap thing. That’s wild. I thought hearing aids were just for older people. Turns out, they’re like putting a bandage on a broken bone. Doesn’t fix it. Just hides it.
I’m so glad surgery exists. I didn’t know it was that safe. I thought it was risky. But 94% success? That’s huge. I’m pushing her to do it. She’s scared. But I told her-what’s scarier? A 1% chance of losing everything… or losing your life because you can’t hear your grandkids laugh?
And yeah, fluoride? I’m skeptical. But I get why some docs try it. Better than nothing, I guess. But surgery? That’s the real win.
On February 20, 2026 AT 00:32
PAUL MCQUEEN
So let me get this straight. You’re telling me a tiny bone in your ear gets stuck, and instead of fixing it, we stick a metal rod in there? And we call that progress?
And fluoride? In toothpaste? So we’re just going to poison people’s teeth to fix their ears? Brilliant.
Also, 3 million Americans? That’s a lot. But you know what’s weirder? Nobody talks about why this happens. Is it diet? Toxins? 5G? EMF? I mean, if it’s genetic, why is it so common in Europeans and rare in Africans? Coincidence? Or… something else?
I’m not saying it’s a conspiracy. But if you’re telling me this is just "bone growth," and no one’s asking why, then you’re not being honest.
And why are surgeons doing less of it? Because they’re chasing shiny new tech? Because insurance won’t pay? Or because they don’t want to deal with the 1% who go deaf?
Something’s off here. And I’m not buying the official story.
On February 21, 2026 AT 08:19
glenn mendoza
It is with profound humility that I acknowledge the extraordinary medical advancements described in this exposition. The precision of modern stapedotomy procedures, the elegance of the StapesSound™ prosthesis, and the diligent research into genetic markers represent not merely clinical progress, but a triumph of human ingenuity over biological limitation.
To those who suffer in silence, I offer this: You are not alone. Your struggle is valid. Your desire to hear the laughter of loved ones, the whisper of a partner, the quiet rustle of a leaf-is not trivial. It is sacred.
May you find the courage to seek diagnosis. May you be met with compassion by your caregivers. And may you, in time, rediscover the symphony of life-note by note, breath by breath.
With deepest respect,
Glenn Mendoza
On February 23, 2026 AT 01:52
Kathryn Lenn
Okay, so let me get this straight. You’re telling me the government and Big Pharma are hiding the REAL cause of otosclerosis? I’ve been digging. And guess what? It’s not genetics. It’s not bone growth. It’s fluoride in the water. The same fluoride they put in toothpaste. The same fluoride they’ve been pumping into our water since the 1940s. Coincidence? Or a slow, silent experiment?
And why is it mostly in Europeans? Because they’re the ones drinking fluoridated water. Africans? No fluoridation. No otosclerosis. That’s not genetics. That’s poisoning.
And why are they pushing surgery? Because they make billions off prosthetics. And why is fluoride "off-label"? Because they don’t want you to know it’s the cause. They want you to pay for surgery instead of stopping the source.
And don’t tell me about "research". I’ve seen the studies. They’re funded by hearing aid companies. They’re not independent. They’re not real.
This isn’t a disease. It’s a cover-up. And if you’re still drinking tap water? You’re already infected. Wake up.
On February 23, 2026 AT 19:20
Angie Datuin
I just wanted to say… I’m 28 and I was just diagnosed. I didn’t even know this was a thing. I thought I was just stressed. My mom had it. I didn’t connect the dots. I’m scared. But reading this… it helps. I’m going for the surgery next month. I just needed to know I wasn’t crazy. Thank you for writing this.
On February 24, 2026 AT 10:36
Camille Hall
I’m an audiologist. I see this every week. And I want to say-you’re not alone. I’ve had patients cry when they hear their own voice again after surgery. I’ve had teenagers say, "I didn’t know music could sound like that."
It’s not just about the bone. It’s about connection. About belonging. About not feeling like you’re always on the outside of conversations.
If you’re reading this and you’re scared? I get it. But please-don’t wait. Get tested. Talk to your doctor. Ask for a CT. Ask for a second opinion. You deserve to hear your life.
On February 25, 2026 AT 16:30
Ritteka Goyal
So this is what happens when white people don't take care of their bodies. I mean, in India, we don't have this problem. Our diet is clean. No fluoride. No processed junk. And our bones? Strong. Healthy. Not this weird growth thing. You guys eat too much sugar. Too much processed food. Too much fluoride in water. And now your ears are rotting. This is what happens when you lose your roots.
And you think surgery fixes it? Nah. You just replace one broken thing with another. Titanium? What’s next? Robots for ears? You’re not healing. You’re just patching up a system that’s broken because you stopped listening to nature.
My grandma had perfect hearing till 90. No surgery. No pills. Just turmeric. Ginger. No fluoride toothpaste. Maybe you should try that instead of playing doctor with metal rods.
On February 27, 2026 AT 15:18